For US healthcare professionals only
Director, Hypertrophic Cardiomyopathy Center
Co-Director, Cardiac CT and MRI
Assistant Professor, Tufts University School of Medicine
Boston, MA
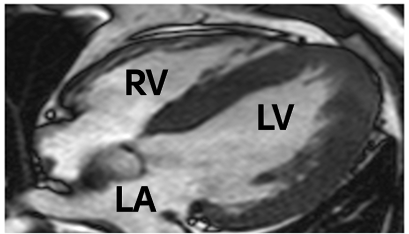
A 12-lead electrocardiogram (ECG) showed diffuse T-wave inversion, prominent in lateral precordial leads V4-V6, and associated with tall R-waves and normal PR interval. Echocardiographic and cardiovascular magnetic resonance imaging showed an ejection fraction of 70%, with a symmetric pattern of left ventricular hypertrophy in which all segments of the wall were equally involved in the hypertrophic process, measuring 17 to 19 mm. The contiguous right ventricular wall was also hypertrophied (ie, 10 mm). Systolic anterior motion of the mitral valve was absent, and left ventricular outflow velocities were normal, consistent with the nonobstructive state.1
The patient was identified as having Fabry disease during a screening program in which all patients had alpha-Gal A enzyme activity testing followed by analysis of GLA, the gene coding for alpha-Gal A, in males with low enzyme activity and most females.1 This patient’s GLA variant (N215S) is one frequently associated with cardiac disease, and he lacked noncardiac manifestations of Fabry disease (had a cardiac variant presentation).1
One year after Fabry disease diagnosis, an implantable cardioverter-defibrillator was implanted owing to a family history of sudden cardiac death. Within 24 hours the implantable cardioverter-defibrillator interrupted ventricular fibrillation with a 35J shock.1 Family cascade screening identified 11 additional family members with Fabry disease. The patient and six additional family members began Fabry disease–specific therapy.1
GLA, galactosidase alpha gene; LA, left atrium; LV, left ventricle; RV, right ventricle.
Reference: 1. Maron MS, Xin W, Sims KB, et al. Identification of Fabry disease in a tertiary referral cohort of patients with hypertrophic cardiomyopathy. Am J Med. 2018;131(2):200.e1-200.e8.