For US healthcare professionals only
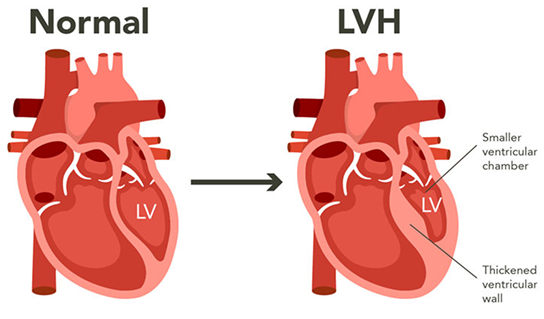
GL-3 accumulation in cardiomyocytes can lead to unexplained, progressive left ventricular hypertrophy (LVH), either as an isolated finding or in conjunction with other Fabry disease symptoms.2,3 LVH in Fabry disease typically combines concentric thickening with absent or minimal left ventricular obstruction and normal left ventricular ejection fraction. However, asymmetric septal or atypical hypertrophy has also been described, along with subaortic obstruction, which may mimic the phenotypical and clinical features of sarcomeric HCM.3
The high incidence of LVH in Fabry disease leads to difficulty in distinguishing Fabry disease from sarcomeric HCM.1 In multiple studies, from <0.5% to 1%, and sometimes even up to 4% of patients in HCM, populations have been subsequently diagnosed with Fabry disease.1 The varying percentages are likely influenced by differences in population, diagnostic methods, and other variables.1 Due to the difficulty in diagnosing Fabry disease, a diagnosis of a single family member is often followed by diagnosis of additional family members due to family cascade screening.1,6
In light of its distinctive genetic causes, treatments, and requirement for expert multidisciplinary care, Fabry disease must be differentiated from sarcomeric HCM.3 To reduce misdiagnosis, it has been recommended that7:
Cardiac symptoms are reported in approximately 40% to 60% of patients with Fabry disease, and cardiac complications are the most common cause of mortality.8-10 These facts add importance to timely diagnosis and management of cardiac disease in Fabry disease.11
GL-3 accumulation is not the sole pathogenic factor; rather, it triggers a cascade of secondary processes that may result in inflammation, cell dysfunction, and potentially irreversible tissue damage.8 Fibrosis and involvement of conduction tissue underlie the development of ventricular arrhythmias and conduction disturbances.2 A range of other cardiac manifestations may occur, including myocardial ischemia and infarction as well as chronotropic incompetence.2,8 Progression may result in heart failure, predominantly with preserved ejection fraction.11
Some patients with the late-onset cardiac variant will present with only cardiac symptoms, often LVH that is unexplained by abnormal cardiac loading conditions and/or conduction abnormalities, while other patients will present with signs and symptoms in multiple organ systems.3,7,11 In either case, recognition and diagnosis of Fabry disease, including differentiation from other causes of LVH, are crucial.2
GL-3, globotriaosylceramide; LV, left ventricle.
References: 1. Maron MS, Xin W, Sims KB, et al. Identification of Fabry disease in a tertiary referral cohort of patients with hypertrophic cardiomyopathy. Am J Med. 2018;131(2):200.e1-200.e8. 2. Pieroni M, Moon JC, Arbustini E, et al. Cardiac involvement in Fabry disease: JACC review topic of the week. J Am Coll Cardiol. 2021;77(7):922-936. 3. Hagège A, Réant P, Habib G, et al. Fabry disease in cardiology practice: literature review and expert point of view. Arch Cardiovasc Dis. 2019;112(4):278-287. 4. Antezana-Chavez E, Cianciulli TF, Hadid CL, et al. Value of electrocardiography to distinguish Fabry disease from sarcomeric hypertrophic cardiomyopathy. Am J Cardiol. 2022;178:131-136. 5. Geske JB, Jouni H, Aubry MC, Gersh BJ. Fabry disease with resting outflow obstruction masquerading as hypertrophic cardiomyopathy. J Am Coll Cardiol. 2014;63(17):e43. 6. Laney DA, Fernhoff PM. Diagnosis of Fabry disease via analysis of family history. J Genet Couns. 2008;17(1):79-83. 7. Monda E, Falco L, Palmiero G, et al. Cardiovascular involvement in Fabry’s disease: new advances in diagnostic strategies, outcome prediction and management. Card Fail Rev. 2023;9:e12. 8. Germain DP. Fabry disease. Orphanet J Rare Dis. 2010;5:30. 9. Mehta A, Clarke JTR, Giugliani R, et al; FOS Investigators. Natural course of Fabry disease: changing pattern of causes of death in FOS – Fabry Outcome Survey. J Med Genet. 2009;46(8):548-552. 10. Waldek S, Patel MR, Banikazemi M, Lemay R, Lee P. Life expectancy and cause of death in males and females with Fabry disease: findings from the Fabry Registry. Genet Med. 2009;11(11):790-796. 11. Pieroni M, Namdar M, Olivotto I, Desnick RJ. Anderson-Fabry disease management: role of the cardiologist. Eur Heart J. 2024;45(16):1395-1409.