For US healthcare professionals only
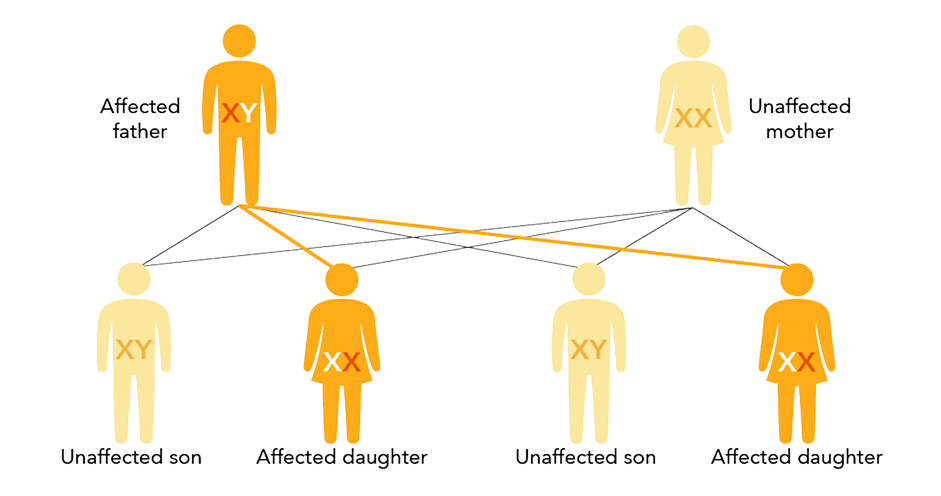
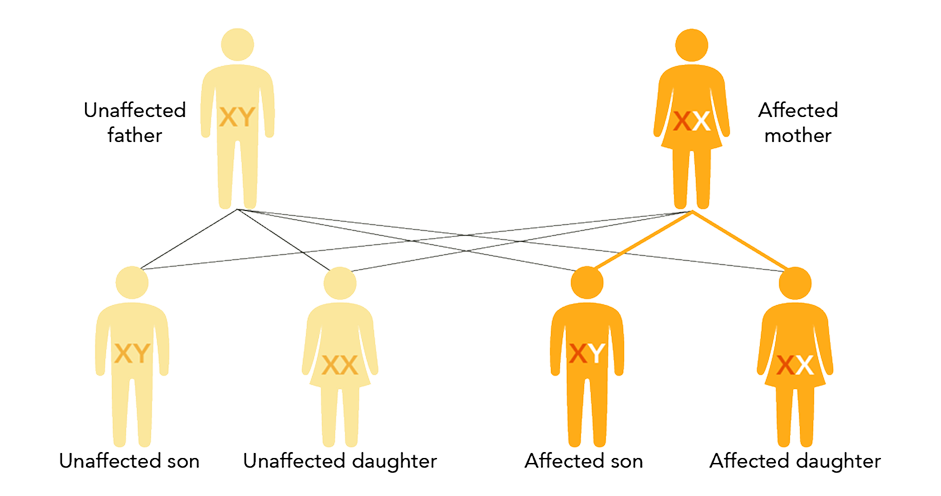

A website, the Fabry Family Tree, is available to help patients diagnosed with Fabry disease and their family members understand the inheritance of Fabry disease and evaluate their risk of having the disease. Patients can build a family tree online and determine whether a family member may share the disease-causing variant.
GLA, galactosidase alpha gene.
References: 1. Germain DP. Fabry disease. Orphanet J Rare Dis. 2010;5:30. 2. ThinkGenetic Foundation. Fabry disease. Accessed April 27, 2025. https://thinkgenetic.org/diseases/fabry-disease 3. Ortiz A, Germain DP, Desnick RJ, et al. Fabry disease revisited: management and treatment recommendations for adult patients. Mol Genet Metab. 2018;123(4):416-427. 4. El-Abassi R, Singhal D, England JD. Fabry’s disease. J Neurol Sci. 2014;344(1-2):5-19. 5. Filoni C, Caciotti A, Carraresi L, et al. Functional studies of new GLA gene mutations leading to conformational Fabry disease. Biochim Biophys Acta. 2010;1802(2):247-252. 6. Gal A. Molecular genetics of Fabry disease and genotype-phenotype correlation. In: Elstein D, Altarescu G, Beck M, eds. Fabry Disease. Springer Science and Business Media; 2010:3-19. 7. Tuttolomondo A, Simonetta I, Duro G, et al. Inter-familial and intra-familial phenotypic variability in three Sicilian families with Anderson-Fabry disease. Oncotarget. 2017;8(37):61415-61424. 8. Knol IE, Ausems MGEM, Lindhout D, et al. Different phenotypic expression in relatives with Fabry disease caused by a W226X mutation. Am J Med Genet. 1999;82(5):436-439. 9. Hoffmann B, Mayatepek E. Fabry disease—often seen, rarely diagnosed. Dtsch Arztebl Int. 2009;106(26):440-447. 10. Marchesoni CL, Roa N, Pardal AM, et al. Misdiagnosis in Fabry disease. J Pediatr. 2010;156(5):828-831. 11. Pieroni M, Namdar M, Olivotto I, Desnick RJ. Anderson-Fabry disease management: role of the cardiologist. Eur Heart J. 2024;45(16):1395-1409. 12. Reisin R, Perrin A, García-Pavía P. Time delays in the diagnosis and treatment of Fabry disease. Int J Clin Pract. 2017;71(1):e12914. 13. Wilcox WR, Oliveira JP, Hopkin RJ, et al. Females with Fabry disease frequently have major organ involvement: lessons from the Fabry Registry. Mol Genet Metab. 2008;93(2):112-128. 14. Echevarria L, Benistan K, Toussaint A, et al. X-chromosome inactivation in female patients with Fabry disease. Clin Genet. 2016;89(1):44-54.